
Urinary Tract Infection in Women
Symptoms, Causes, Pregnancy, Recurrent UTI, Treatment, and Prevention
Reviewed by Dr. Pallavi Kulkarni, MBBS, DGO, DNB (OB-GYN), DFP, Fellowship in IVF, MRCOG (Royal College of Obstetricians and Gynaecologists, UK) ·
If you have ever rushed to the bathroom feeling like you really need to go, only to pass a few painful drops, you already know what a urinary tract infection feels like. UTIs are one of the most common reasons women in Mumbai book a same-day appointment, and yet most patients tell us they tried to ignore it for two or three days first.
The reassuring part is that an uncomplicated UTI is straightforward to test for and usually clears with a short course of the right antibiotic. The trickier part is knowing when it is “just a UTI,” when it is something more serious, and what to do if it keeps coming back.
At Aarogya Women’s Clinic in Kandivali East, Dr. Pallavi Kulkarni sees UTIs across every life stage: newly married women, working professionals, women in pregnancy, and women after menopause. The pattern is different in each group, and so is the right treatment.
This page explains what a UTI is, why women get them more often than men, what to watch for, how UTIs in pregnancy are managed differently, what to do about recurrent infections, and how to lower your risk in everyday life.
Part of our gynecological infections cluster, and sits alongside our pages on vaginal discharge and fungal infection in women.

“Most of my patients arrive on day three. They have already tried drinking more water, they have hoped it would settle, and now the burning has not gone away. The honest answer is that a UTI rarely settles on its own, and the longer it sits, the higher the risk that it climbs up to the kidneys. A urine test and the right antibiotic, started early, fix this in days.”
- Dr. Pallavi Kulkarni
Do I need to see a doctor today?
| Your situation | What to do |
|---|---|
| Burning or frequency, no fever, not pregnant | See a doctor today or tomorrow. Same-day urine test advised. |
| Fever, chills, or back/flank pain alongside burning | Urgent same-day evaluation. Do not wait. Call now. |
| Pregnant and any urinary symptom (even mild) | See your doctor today. UTIs in pregnancy are treated even when mild. |
| Postmenopausal with a 2nd or 3rd UTI in a few months | Book a consultation. Recurrent UTI in this group has specific options beyond antibiotics. |
What Is a UTI and Why Does It Happen More in Women?
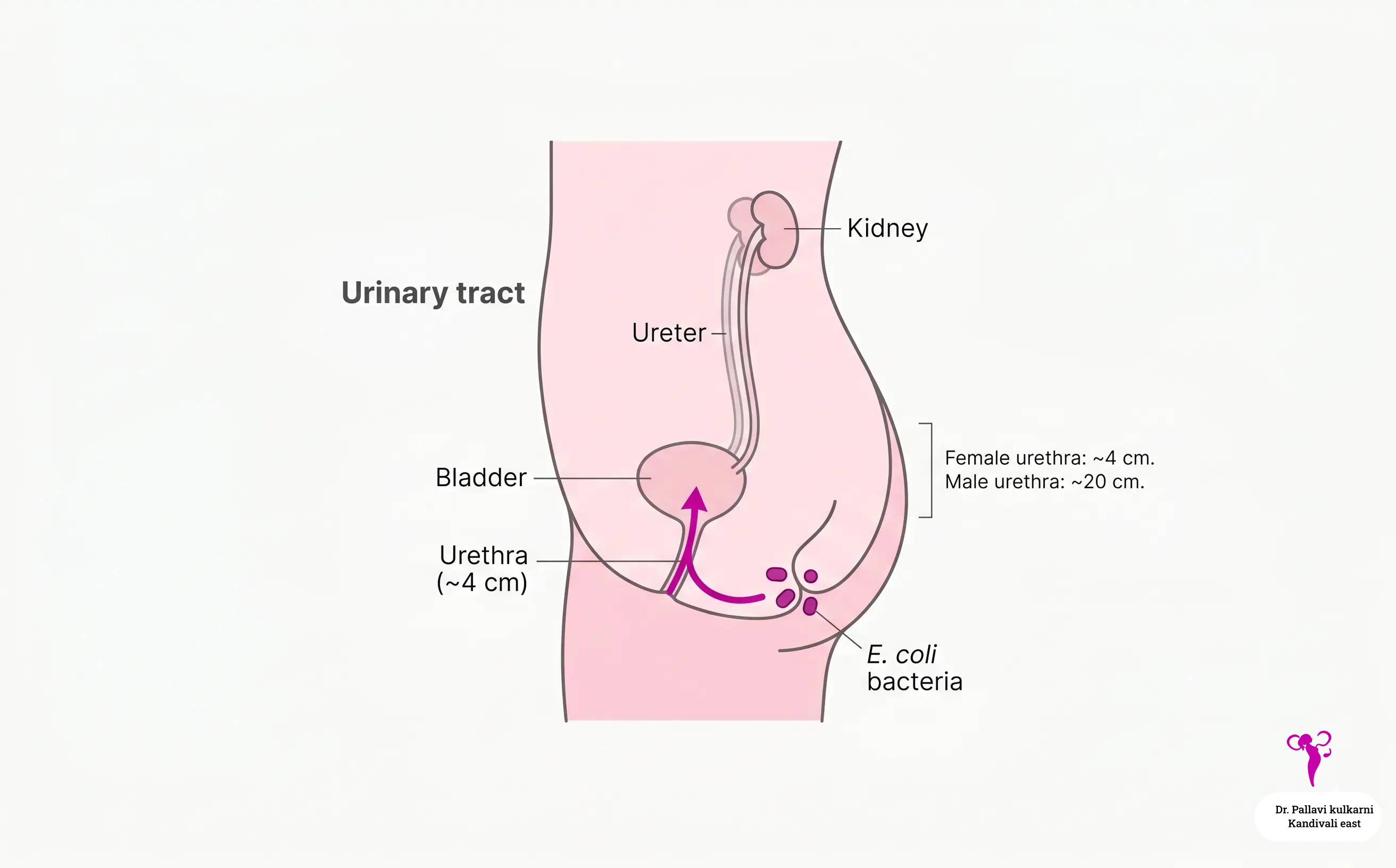
The urinary tract is the system that makes, stores, and passes urine. It includes the kidneys at the back, two long tubes called ureters that carry urine down to the bladder, the bladder itself in the lower abdomen, and a final short tube called the urethra that lets urine out of the body.
A urinary tract infection happens when bacteria, almost always from the bowel, find their way into this system and start to multiply. The result is inflammation, irritation, and the symptoms most women know all too well. The NHS overview of urinary tract infections is a useful plain-English summary if you want a second source alongside this page.
Why women get UTIs more often than men
The female urinary system is genuinely more exposed than the male one, and that is not your fault. There are three anatomical reasons:
- The female urethra is short. It is roughly 4 cm long in women, compared to about 20 cm in men. That short distance is all the bacteria have to travel to reach the bladder.
- The opening of the urethra sits very close to the vagina and the anus. Bacteria that normally live around the anus do not have far to go.
- Sexual intercourse can mechanically push bacteria toward the urethra. This is why some women develop a UTI within 24 to 48 hours of sex, sometimes called “honeymoon cystitis.”
Pregnancy, menopause, diabetes, and certain types of contraception (such as diaphragms and spermicides) all add to the risk on top of the basic anatomy.
How Common Are UTIs in Indian Women?
UTIs are one of the most frequent bacterial infections seen in women of all ages. Globally, around half of all women will have at least one UTI in their lifetime, and many will have more than one.
Two practical takeaways from these numbers:
- For most uncomplicated UTIs in Indian women, the cause is E. coli, which is reassuring because it is well understood and well treated.
- Antibiotic resistance, including ESBL-producing strains, is rising in Indian community settings. That makes a urine culture, rather than a guess at the chemist, the safer first step in many cases.
Sources: Mavi et al., systematic review, Cureus, 2024; Hombach M et al., multi-region community uropathogen study, Access Microbiology, 2022.
Types of UTI Women Should Know About
Not every UTI is the same, and the type matters because the urgency, the test, and the treatment all change.
Cystitis (bladder infection)
This is the most common type. The infection sits in the bladder and the urethra. Symptoms are usually classic burning, frequency, urgency, and a dull ache low in the pelvis. Most cases settle quickly with a short antibiotic course.
Urethritis (urethral infection)
When the infection is mostly in the urethra itself, the burning is the loudest symptom and there may be little frequency. In sexually active women, urethritis can sometimes be due to sexually transmitted infections such as chlamydia or gonorrhoea rather than the usual gut bacteria, which is why your doctor may ask about partners and recent intercourse.
Pyelonephritis (kidney infection)
If a bladder infection is left untreated, it can climb up the ureters and reach the kidneys. This is a more serious illness. Typical features are fever, chills, nausea or vomiting, and a deep ache in the flank or lower back, on one side. Pyelonephritis often needs stronger antibiotics, sometimes given as injections, and occasionally hospital admission.
Asymptomatic bacteriuria
Bacteria are present in the urine but the woman feels nothing. In most non-pregnant women this does not need treatment. In pregnancy it does, because untreated bacteriuria carries real risks (covered later on this page).
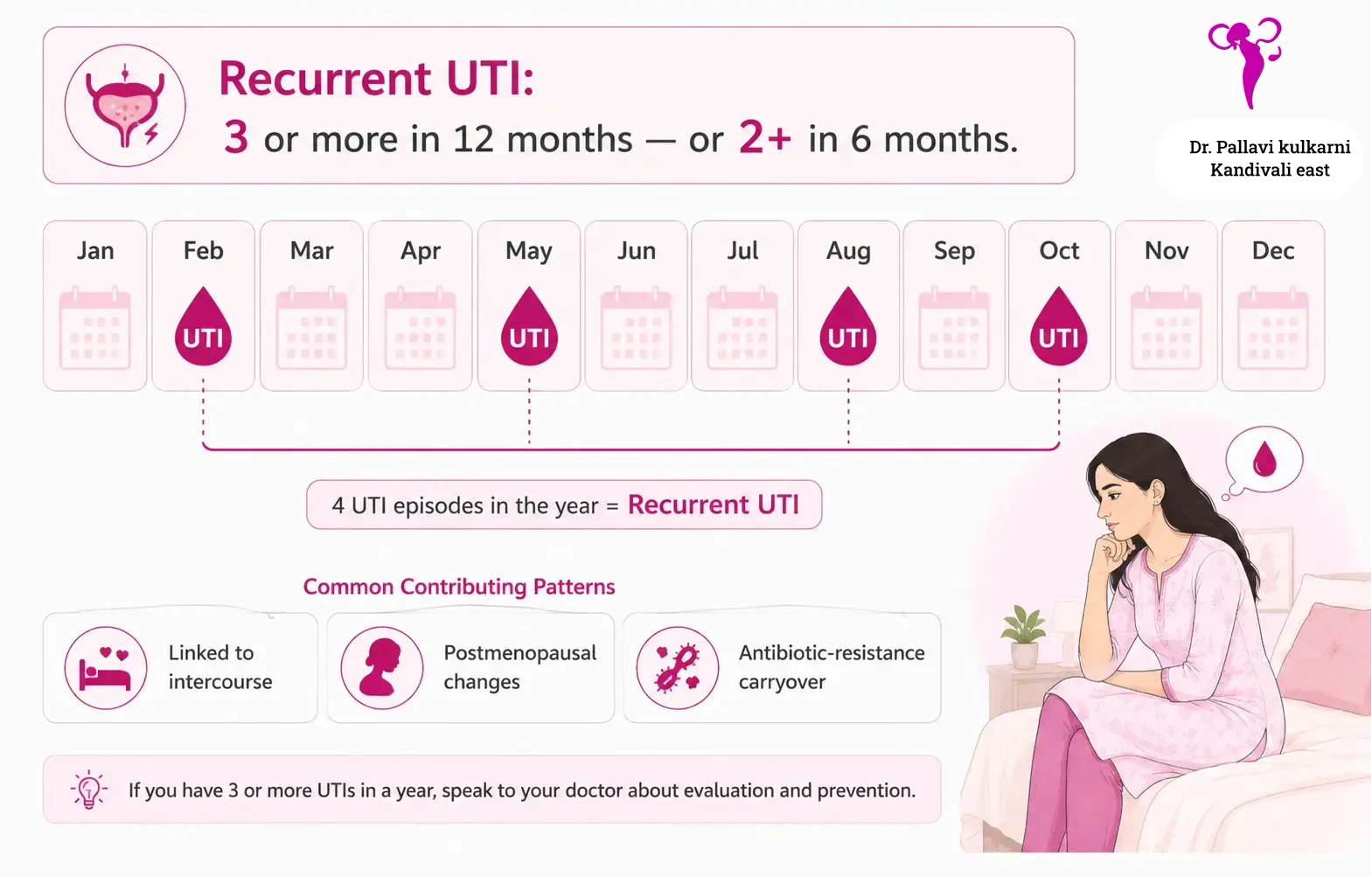
Recurrent UTI
Defined as two or more UTIs in six months, or three or more in a year. Recurrent UTI is its own situation and usually deserves a longer conversation about triggers, prevention, and sometimes preventive medication.
Complicated UTI
This is the term doctors use when a UTI sits on top of something else: pregnancy, diabetes, a kidney stone, structural changes in the urinary tract, a recent catheter, or an immune-suppressing condition. Complicated UTIs are evaluated and treated more carefully than simple cystitis.
What Causes a UTI in Women?
In about 80 to 90 percent of UTIs, the bacteria responsible are bowel bacteria, with E. coli leading the list. They reach the urinary tract by travelling the very short distance from the perineum to the urethral opening.
Common causes and triggers
- Wiping back to front after using the toilet, which carries bowel bacteria toward the urethra.
- Holding urine for long stretches. Urine is your bladder’s natural rinse cycle. The longer urine sits, the more time bacteria have to settle and multiply.
- Sexual activity. Intercourse mechanically moves bacteria toward the urethra. Newly sexually active women, including newly married women, are particularly vulnerable in the first few weeks or months.
- Dehydration, which leads to less frequent urination and more concentrated urine. Mumbai humidity and air-conditioned offices are a quiet contributor here.
- Pregnancy. Hormonal and mechanical changes (covered separately below).
- Menopause and low estrogen, which thins the lining of the urethra and vagina and changes the bacterial balance.
- Diabetes, especially if blood sugar is not well controlled.
- Constipation, which keeps a higher load of gut bacteria sitting close to the urethra.
- Use of diaphragms, spermicides, or unlubricated condoms.
- Catheter use, even short-term, in hospital.
- Kidney stones or any obstruction that blocks the normal flow of urine.
Causes that are over-blamed
Most “common knowledge” about UTI causes mixes truth with folklore. A few quick clarifications:
- Sitting on a public toilet seat does not cause a UTI on its own. The bacteria need to be carried to the urethra, usually via wiping or hands, not absorbed from the seat.
- Wearing the same panty for too long does not directly cause a UTI, but a damp environment can encourage bacterial growth around the urethra and vagina.
- Cold weather or “cooling foods” do not cause UTIs in any meaningful way.
- A single, isolated UTI does not mean your immune system is weak.
Symptoms of UTI in Women
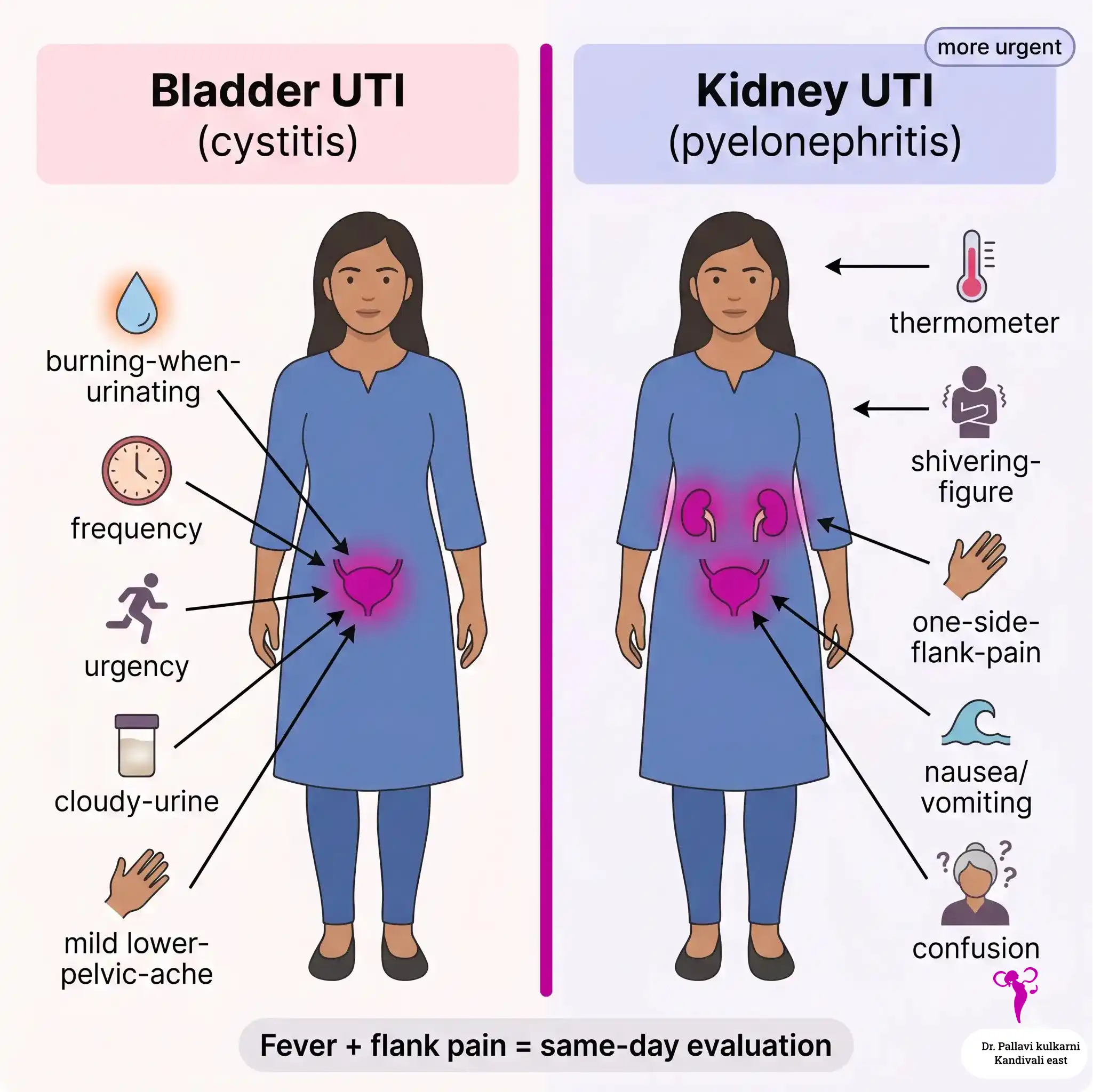
UTI symptoms are usually obvious once you know what you are looking for. The challenge is telling a bladder infection apart from a kidney infection, because the second one is more urgent.
In clinic, most women who walk in with a UTI describe the same four things, often in this order: a burning or pain while passing urine, a frequent urge to urinate, passing only small amounts of urine each time, and a lower abdominal pain or pressure.
When three or four of these are present together, especially in an otherwise well woman with no fever, it almost always points to an uncomplicated bladder infection. A urine test confirms it and a short course of the right antibiotic, started early, settles it in two to three days. The cases that need quicker attention are the ones where fever, chills, or one-sided back pain join in, because that suggests the infection has begun to climb upward.
- Dr. Pallavi Kulkarni, on patterns frequently seen in UTI consultations at Aarogya Women’s Clinic
| Bladder UTI (cystitis) | Kidney UTI (pyelonephritis) |
|---|---|
| Burning or stinging when passing urine | All of the bladder symptoms, plus the ones below |
| Strong, frequent urge to urinate | Fever (often above 38°C / 100.4°F) |
| Passing only small amounts at a time | Chills or shivering |
| Cloudy, dark, or strong-smelling urine | Pain in one flank, lower back, or just under the ribs |
| Mild lower abdominal or pelvic ache | Nausea or vomiting |
| Sometimes a trace of blood in urine | Feeling generally unwell, weak, or shaky |
| Usually no fever | New confusion (in older women) |
Two important points about symptoms:
- In older women, particularly women over 70, a UTI can present mostly as new confusion, sudden tiredness, or a fall, with very few classic urinary symptoms. If your mother or grandmother becomes unusually confused, a urine test is worth doing.
- A trace of pink or red in your urine on its own is not always a UTI. It can also point to a bladder issue, a kidney stone, or sometimes a more important problem. Visible blood in urine should always be evaluated.
“When a woman calls and says ‘it is just the burning,’ I am usually relaxed. When she says ‘I have a fever and my back hurts on one side,’ I move that appointment up. The difference between cystitis and pyelonephritis is hours, not days.”
- Dr. Pallavi Kulkarni
Burning when you urinate, or a fever with back pain that started today? A urine test and the right antibiotic on day one is far easier than catching up on day five.
When a UTI Becomes an Emergency
Most UTIs are not emergencies, but some are. Please go to a hospital, or call us straight away, if you have:
- A high fever with chills, especially with back or flank pain
- Severe nausea or repeated vomiting that stops you keeping fluids down
- Visible blood in the urine, or clots
- A racing heart, breathlessness, or feeling faint
- A UTI in pregnancy, especially with any fever
- A UTI in a woman with diabetes, kidney disease, or a transplant
- A UTI in a woman who has recently had a urinary catheter or a urological procedure
- Any new confusion or drowsiness in an older woman, even without obvious urinary symptoms
These features can signal pyelonephritis or, more rarely, urosepsis, where the infection enters the bloodstream. Both are treatable, but they are more easily treated early.
UTI in Pregnancy: Why It Matters More
Pregnancy changes how the body handles bacteria in the urinary tract, in three ways. Hormones (mainly progesterone) relax the muscle of the ureters, slowing the flow of urine. The growing uterus presses on the bladder and can keep some urine sitting back. And changes in immune tolerance during pregnancy make it slightly easier for an infection to take hold.
The result is that pregnant women are at higher risk of UTIs, and even bacteria found “by accident” in a routine urine test (asymptomatic bacteriuria) need treatment. This is one of the few situations in adult women where a urine that has not caused any symptoms is still treated.
Why pregnancy UTIs need extra attention
Untreated UTIs in pregnancy are associated with:
- Pyelonephritis, which is more common and more serious in pregnancy
- Preterm labour and preterm birth
- Low birth weight
- Higher risk of admission for the mother
Most of these risks drop sharply with timely antibiotic treatment. This is why a urine test is part of the routine first-trimester pregnancy care check, and why it is repeated through pregnancy if the first one shows bacteria, or symptoms appear later.
Antibiotic choice in pregnancy
Antibiotic selection in pregnancy is careful, because not every antibiotic is safe across every trimester. As a general guide, nitrofurantoin and certain penicillins and cephalosporins are commonly used. Trimethoprim-containing combinations are avoided in the first trimester. Fluoroquinolones (ciprofloxacin, norfloxacin) and tetracyclines are not used in pregnancy. The exact choice depends on culture results, gestation, and your medical history, which is why pregnancy UTIs are not a place for chemist-counter self-treatment.
If you have had a UTI in this pregnancy, you may also be reviewed under our high-risk pregnancy care protocol if there is a kidney infection or a recurrent pattern.
Pregnant and feel a burning when you urinate? Please do not wait this one out. A same-day urine test and the right antibiotic protect both you and the baby.
Recurrent UTI: When It Keeps Coming Back
If you have had two UTIs in six months, or three or more in twelve months, you fit the medical definition of recurrent UTI. This is more common than people realise, particularly in two groups: women who are sexually active and women after menopause.
Why recurrent UTIs happen
Several patterns sit behind recurrent infection:
- Repeated reinfection from gut bacteria, often related to sexual activity, wiping habits, or low fluid intake
- Incomplete bladder emptying, where some urine is left behind every time you go
- Postmenopausal changes in the vaginal and urethral lining, which alter the local bacterial balance
- Bacterial biofilms that protect themselves from antibiotics and re-emerge a few weeks later
- Antibiotic resistance, where the original UTI was treated with an antibiotic the bacteria were partly resistant to, and a small population survived
- An underlying issue such as a kidney stone or a structural change in the urinary tract
How recurrent UTI is evaluated
A first step is to send a proper midstream urine for culture and sensitivity, ideally before any antibiotic is started, so that the actual bacterium and the right antibiotic are known. A pelvic ultrasound is often added to look at the kidneys and the bladder. In some cases, a measurement of how much urine is left in the bladder after you urinate (a post-void residual) is helpful.
What can be done about recurrent UTIs
There is more to offer than just another antibiotic. Depending on your pattern, options include:
- Targeted antibiotic therapy based on the culture, rather than empirical guessing
- Post-coital antibiotic prophylaxis if UTIs are clearly linked to intercourse: a single low-dose tablet taken after sex
- Continuous low-dose prophylaxis for selected patients, usually for three to six months
- Topical estrogen (a small cream or pessary used vaginally) for postmenopausal women, which can reduce recurrence significantly
- Vaginal probiotics, with reasonable evidence for some strains
- Cranberry-based products (juice, capsules, or D-mannose), which the Cochrane review suggests may reduce recurrence in some women, though the evidence is mixed and they should not be used as a treatment for an active infection
- Behavioural changes that genuinely make a difference, listed in the prevention section below
- Referral to a urologist if structural causes are suspected
The right combination depends on the woman, not on a textbook list.
Watch: Dr. Pallavi on breaking the recurrent-UTI cycle
~9 minutes. Watch on YouTube: Recurrent UTI in Women - Why It Keeps Coming Back & How to Stop the Cycle
UTI After Menopause
Many women are surprised to find that UTIs become more frequent after menopause. Postmenopausal UTI behaves differently from a typical 30-something cystitis pattern - the trigger is not usually intercourse or hydration, it is the hormonal change itself - and it responds to a different treatment approach.
Why menopause raises UTI risk
As estrogen levels fall after the menopause, the lining of the vagina and the urethra becomes thinner, drier, and less elastic - a condition known as genitourinary syndrome of menopause. Three things change at the same time. The local vaginal pH rises from the typical reproductive-age 3.5 to 4.5 toward 6 or higher. The protective lactobacilli that keep gut bacteria in check decline sharply. And the bladder muscle may empty less completely, leaving residual urine in which bacteria can multiply. The combined effect is that E. coli and other organisms colonise the periurethral area more easily and ascend to the bladder more often.
What treatment actually works
The standard approach in this group is not an indefinite stream of antibiotics. Vaginal estrogen - given as a small cream or pessary used twice a week - is the most effective preventive measure for postmenopausal recurrent UTI. It restores the vaginal lining and the lactobacilli, which restores the natural protection. Very little of the hormone reaches the bloodstream, so the safety profile is good even for women who cannot take systemic hormone therapy.
Alongside vaginal estrogen, a urine culture before each new antibiotic course (rather than empirical guessing), good hydration, and treatment of constipation if present, often bring the frequency down from every two to three months to once a year or less.
When to ask about vaginal estrogen
If you are postmenopausal and have had two or more UTIs in the last six months, or three or more in the last year, please mention it at your consultation. It is the right moment to discuss vaginal estrogen, even if you have never used hormone therapy before. This is something we cover in detail at our menopause clinic, alongside the other genitourinary symptoms (vaginal dryness, painful intercourse, urinary urgency) that frequently travel with recurrent UTIs in this age group.
Postmenopausal and your UTIs are coming back? A consultation at our Menopause Clinic in Kandivali East can review whether vaginal estrogen is right for you.
How Are UTIs Diagnosed?
Diagnosis is usually quick. The tests below are chosen based on whether this is a one-off UTI, a UTI in pregnancy, or a recurrent or complicated UTI.
| Test | What it tells us |
|---|---|
| Urine dipstick (in the clinic) | A bedside test that screens for nitrites, leukocyte esterase, blood, and protein. A positive nitrite or leukocyte test in a symptomatic woman strongly supports a UTI. |
| Urine routine and microscopy | A laboratory examination of the urine for white cells, red cells, and bacteria. Confirms the dipstick finding. |
| Urine culture and sensitivity | The gold standard. Identifies the exact bacterium and which antibiotics it is sensitive or resistant to. Always done in pregnancy, recurrent UTI, suspected pyelonephritis, and treatment failure. |
| Blood tests | Used in suspected pyelonephritis or unwell patients: complete blood count, CRP, kidney function, blood culture in some cases. |
| Pelvic and renal ultrasound | Looks at the kidneys, ureters, and bladder. Used in recurrent UTI, suspected stones, suspected pyelonephritis, or pregnancy where imaging is needed. |
| Post-void residual | Measures how much urine remains in the bladder after you go. Helpful if incomplete emptying is suspected. |
| Cystoscopy or further imaging | Reserved for selected complicated or recurrent cases, usually after a urology referral. |
For most uncomplicated UTIs in non-pregnant women, a urine sample and a clinical examination are enough to start treatment the same day. A culture is sent in parallel where appropriate, and the treatment is adjusted later if the bacterium turns out to need a different antibiotic.
How to give a clean urine sample
A common reason a urine result looks confusing is contamination. A few simple steps make the test much more reliable:
- Wash your hands first.
- Use the cleansing wipe provided, front to back, before passing urine.
- Pass the first part of the stream into the toilet, then collect the middle part into the container, then finish into the toilet. This is called a midstream sample.
- Close the lid promptly and hand it in within an hour where possible.
How Are UTIs Treated?
The mainstay of treatment is the right antibiotic, in the right dose, for the right number of days. Self-medication and chemist-counter antibiotics are one of the main reasons UTIs come back, because the wrong antibiotic, or a half course, leaves resistant bacteria behind.
First-line antibiotics for uncomplicated UTI
International guidance from the Infectious Diseases Society of America and the European societies recommends nitrofurantoin, fosfomycin, and trimethoprim-sulfamethoxazole as first-line options for uncomplicated cystitis, with the local choice guided by what E. coli in the area is sensitive to. Fluoroquinolones such as ciprofloxacin and norfloxacin, often the first thing handed out at a chemist in India, are deliberately not first-line for an uncomplicated UTI in the current guidelines, both because of side effect concerns and because overusing them drives resistance for everyone.
A typical course is three to seven days for cystitis, depending on the antibiotic. Symptoms usually improve within 24 to 48 hours of starting the right tablet, but the course should be completed.
Treatment for kidney infection
Pyelonephritis is treated more aggressively. Mild cases may be managed with oral antibiotics for ten to fourteen days. More unwell women, pregnant women, women who cannot keep fluids down, or those with diabetes or other risk factors are often started on intravenous antibiotics, sometimes with a short hospital stay.
Symptom relief while antibiotics work
Alongside the antibiotic, a few simple measures help:
- Drink more water than usual, enough to keep urine pale.
- Paracetamol for pain or fever, in standard doses, is generally safe.
- Avoid coffee, alcohol, and very spicy food for a few days, as they can irritate the bladder.
- Rest. UTI symptoms feel disproportionate to how unwell women look, and rest helps.
What to expect, day by day
- Day 1. Burning, frequency, urgency, sometimes a low-grade ache. Antibiotic started.
- Days 2 to 3. Symptoms ease noticeably for most women.
- Day 4 to end of course. Symptoms usually settled. Continue the tablets.
- A week after finishing. Most women feel back to normal. A repeat urine test may be done in pregnancy, recurrent UTI, or if symptoms have not fully resolved.
If symptoms have not started easing by day three, the antibiotic may not be matching the bacterium. Please call rather than waiting it out: a culture result usually clarifies the next step.
Antibiotic Resistance in India: Why Self-Medication Is Risky
Antibiotic resistance in urinary pathogens is a real and growing problem in India. Studies of community UTIs across the country have found high rates of resistance to the very antibiotics most often bought over the counter, including ciprofloxacin, norfloxacin, and ampicillin, with ESBL-producing E. coli and Klebsiella now present in a meaningful fraction of community samples.
The everyday consequence: a tablet that worked for your friend, or for you a year ago, may not work today. The right way through this is not to despair but to use the tools we have:
- A urine culture before, or alongside, starting antibiotics, particularly in recurrent and pregnancy cases
- Choosing antibiotics based on local sensitivity data
- Completing the full course
- Not pressing for “stronger” antibiotics when a narrower one will do
- Avoiding antibiotics for mild bladder discomfort that has not been confirmed as a UTI
This is also the reason a brief consultation with a doctor, even for a one-off UTI, is genuinely worthwhile. It is a small investment that protects future you.
How to Prevent UTIs
There is no single trick that prevents every UTI, but a small set of habits, kept consistently, brings the rate down for most women. The list below is shaped for an Indian everyday context.

Habits that genuinely help
- Drink water through the day, not all at once. Aim for pale yellow urine. In Mumbai’s heat and humidity, especially during May and the pre-monsoon weeks, fluid loss from sweating is easy to miss.
- Do not hold urine for hours. This is the single hardest habit for working women in offices with limited toilet access, and it is one of the highest-yield changes.
- Wipe front to back. Always.
- Urinate within 15 to 30 minutes after sex. This is the most useful single habit for women whose UTIs are linked to intercourse.
- No washing, no douching - just dab the area dry with a clean tissue. The vagina is self-cleaning. Internal douches and strong intimate washes disturb the natural bacterial balance and increase infection risk, and even repeated plain-water washing through the day strips away the protective layer. After passing urine, simply dab the area dry with a soft tissue. That is enough.
- Use public washrooms carefully. Avoid sitting directly on the seat where you can - use a paper liner or wipe the seat down first. Carry your own pack of soft tissues so you are never relying on what is (or is not) available. Wash your hands before and after, and dab dry rather than scrubbing.
- Cotton, breathable underwear, and not too tight clothing, especially in hot weather.
- Treat constipation seriously, with fibre, fluids, and movement. Chronic constipation keeps bowel bacteria sitting close to the urethra.
- Manage diabetes well. High blood sugar gives bacteria more to feed on.
- For postmenopausal women, discuss vaginal estrogen if UTIs are recurrent. It is one of the most effective preventive measures.
Things people try that are mostly safe but not magic
- Cranberry juice or capsules. Mixed evidence. Probably reduces recurrence somewhat in some women. Reasonable to try, not a substitute for antibiotics in active infection.
- D-mannose powder. Some evidence for prevention of recurrent UTIs. Generally well tolerated.
- Probiotics. Possibly helpful, particularly vaginal probiotics in women with disturbed flora.
Things to avoid
- Self-prescribing antibiotics from a chemist for “just in case” use.
- Strong, perfumed intimate washes and antibacterial soaps in the genital area.
- Holding urine on long bus and train commutes. When you can, plan a stop.
- Ignoring early symptoms in the hope that they pass.
“Patients ask me for one or two changes that make a real difference. My honest answer is two: drink water through your day, and please urinate after sex. If a third is needed, treat constipation properly. These three things prevent more UTIs than any supplement on the shelf.”
- Dr. Pallavi Kulkarni
When to See a Specialist
Please book an appointment if any of the following apply:
- You have classic UTI symptoms (burning, urgency, frequency) that have lasted more than a day or two
- You have a fever, chills, or back or flank pain alongside urinary symptoms
- You see blood in your urine
- You are pregnant and suspect a UTI, even a mild one
- You have had two or more UTIs in the last six months, or three or more in the last year
- You finished an antibiotic course and your symptoms have come back within a few weeks
- You are postmenopausal and your UTIs have started occurring more often
- You have diabetes, kidney disease, or a transplant
- You have had a recent catheter or urological procedure
- An older family member has become unusually confused, tired, or unwell, with or without urinary symptoms
Dr. Pallavi Kulkarni evaluates and treats UTIs as part of her general gynaecology practice at Aarogya Women’s Clinic. Where a urology opinion or further imaging is needed, she co-manages cases with trusted urologists and radiology centres in the Kandivali and Borivali area.
Clinic hours: Monday to Saturday, 10:00 AM to 9:00 PM · Closed Sundays · Languages: English, Hindi, Marathi
Women from Kandivali East including Thakur Village, Kandivali West, Malad East, Malad West, Borivali East, Borivali West, Goregaon East, and Goregaon West consult Dr. Pallavi Kulkarni for diagnosis and treatment of UTIs in women, including UTIs in pregnancy, recurrent UTIs, and UTIs in postmenopausal women.
Dr. Pallavi Kulkarni is registered with the Maharashtra Medical Council, MMC reg. no. 2005/06/2917. She holds an MBBS (KIMS Karad, MUHS), DNB (OB/GYN) (Central Railway Hospital Byculla, Natboard), Fellowship in IVF (AMOGS-MCOG), DGO (CPS Mumbai), DFP (FOGSI), and MRCOG from the Royal College of Obstetricians and Gynaecologists, UK.
Ready to take the next step? Call +91 91366 33062 or message us on WhatsApp to book a UTI consultation with Dr. Pallavi Kulkarni.
References
- Mavi JK, Kumar A, Singh M, et al. Correlates of Urinary Tract Infections Among Women of Reproductive Age in India: A Systematic Review. Cureus. 2024. PMC11107389.
- Hombach M, Asati S, Bhatia M, et al. Prevalence and resistance pattern of uropathogens from community settings of different regions: an experience from India. Access Microbiology. 2022. PMC8941965.
- Gupta K, Hooton TM, Naber KG, et al. International Clinical Practice Guidelines for the Treatment of Acute Uncomplicated Cystitis and Pyelonephritis in Women: A 2010 Update by IDSA and ESCMID. idsociety.org.
- Anger J, Lee U, Ackerman AL, et al. Recurrent Uncomplicated Urinary Tract Infections in Women: AUA/CUA/SUFU Guideline. American Urological Association. auanet.org.
- NHS. Urinary tract infections (UTIs) - overview. nhs.uk.
- Mayo Clinic. Urinary tract infection (UTI) - symptoms and causes. mayoclinic.org.
- Williams G, Hahn D, Stephens JH, et al. Cranberries for preventing urinary tract infections. Cochrane Database of Systematic Reviews. 2023. cochrane.org.
- Royal College of Obstetricians and Gynaecologists (RCOG, UK). Clinical guidelines and patient information on women’s health, including UTI management in pregnancy and the postpartum period. rcog.org.uk.
This page is reviewed periodically by Dr. Pallavi Kulkarni. Last reviewed . Information provided is for educational purposes and not a substitute for professional medical advice.
Do you have any questions?
Request An AppointmentFAQ
Can a UTI go away on its own without antibiotics?
A small minority of mild bladder UTIs do settle on their own with extra fluids and rest, but it is not the safe bet. Untreated UTIs carry a real risk of climbing to the kidneys, and a few days of antibiotics is far easier than a kidney infection. In pregnancy, in recurrent UTI, and in any UTI with fever, antibiotics are not optional.
Does cranberry juice cure a UTI?
No. Cranberry products may help reduce the risk of recurrent UTIs in some women, but they do not treat an active infection. If you already have burning and frequency, drinking cranberry juice is fine, but it is not a substitute for an antibiotic prescribed for the right organism.
How long does a UTI take to clear with antibiotics?
Most women feel a clear improvement within 24 to 48 hours of starting the right antibiotic, with full resolution by the end of a 3 to 7 day course. Kidney infections take longer, usually 10 to 14 days. If you do not feel better by day three, please come back rather than waiting.
Why do I keep getting UTIs?
Recurrent UTIs in women have several common patterns: bacteria reinfecting from the bowel, UTIs linked to sexual activity, postmenopausal changes in the vaginal lining, incomplete bladder emptying, antibiotic resistance, or sometimes an underlying issue like a kidney stone. A urine culture and an ultrasound usually help us understand which pattern is yours, and treatment then becomes much more targeted.
Can a UTI affect my baby during pregnancy?
A treated UTI in pregnancy rarely affects the baby. An untreated UTI in pregnancy is a different story: it is associated with preterm labour, low birth weight, and kidney infection in the mother. This is why we screen for UTIs early in pregnancy and treat them quickly even when symptoms are mild or absent.
Is it safe to have sex during a UTI?
It is not unsafe, but it is uncomfortable, and intercourse can push more bacteria into the urethra and slow your recovery. Most doctors suggest waiting until your symptoms have settled and you have completed (or nearly completed) your antibiotic course.
What is the difference between a UTI and a yeast infection?
A UTI mainly causes burning when you urinate, frequency, and urgency, with little to no vaginal symptoms. A yeast infection mainly causes itching, irritation, and a thick white discharge, with the burning being external rather than from urinating. The two can occur together, which is why a clinical examination matters.
Can a UTI cause back pain?
A bladder UTI usually causes a low pelvic ache rather than back pain. Back or flank pain, especially on one side and especially with fever, suggests the infection has reached the kidney. That is a more urgent situation.
Are over-the-counter UTI tablets from the chemist safe?
The single dose “burning relief” tablets you can buy at a chemist are usually urinary alkalinisers, not antibiotics. They may ease the burning briefly but they do not treat the infection. The antibiotics often handed out without a prescription, particularly fluoroquinolones, are not the recommended first-line treatment for uncomplicated UTI in current international guidance and are partly responsible for the rising resistance we see in India.
Can dehydration cause a UTI?
Dehydration does not cause a UTI on its own, but it raises the risk by reducing how often you urinate, which lets bacteria multiply for longer in the bladder. Steady fluid intake through the day is one of the simplest preventive measures.
Can a UTI cause infertility?
A simple bladder UTI does not cause infertility. The concern is when an infection spreads upward and develops into pelvic inflammatory disease, which can scar the fallopian tubes. This is why we treat suspected upper urinary or pelvic infections promptly and follow up after treatment.
Should I worry about visible blood in my urine?
Yes, please get it checked. Blood in urine during a UTI is not unusual, but it should never be assumed to be only a UTI without a proper test, especially if it persists after treatment, or if there is no burning. A urine test, and sometimes an ultrasound, gives a clear answer.
Is it normal to feel exhausted after a UTI?
A short period of tiredness after a UTI, especially after a kidney infection, is common and usually settles within one to two weeks. If exhaustion drags on, or if you have other symptoms, a follow-up consultation is sensible.
What Our Patients Say
Experienced Gynecologist in Kandivali East with a Patient-Centered Approach
Dr. Pallavi Kulkarni is a highly regarded Gynecologist in Kandivali East, praised for her calm, compassionate, and patient-centered care. Her supportive approach helps women feel heard, respected, and confident about their treatment decisions.