
Thyroid Disorders in Women
Symptoms, Fertility, Pregnancy, Treatment, and Diet
Reviewed by Dr. Pallavi Kulkarni, MBBS, DGO, DNB (OB-GYN), DFP, MRCOG (UK), Fellowship in IVF ·
If you have been told that your thyroid is “a little off,” or you have been struggling with tiredness, irregular periods, or trouble conceiving, you are not alone. Thyroid disorders are one of the most common hormonal problems in Indian women, and they often go undetected for years.
The reassuring part is that most thyroid disorders in women are easy to test for and very treatable. A simple blood test, the right medication, and a few sensible food and lifestyle adjustments are usually enough to get you back to feeling like yourself.
At Aarogya Women’s Clinic in Kandivali East, Dr. Pallavi Kulkarni evaluates and manages thyroid problems in the context of women’s health, with a particular focus on fertility, pregnancy, and the overlap with conditions like PCOS, irregular periods, and hormonal imbalance.
This page explains what the thyroid is, what symptoms to watch for, how thyroid problems affect fertility and pregnancy, what tests and treatments to expect, and what to eat (and avoid) when you are managing the condition. It is written for women, not for doctors, so the language stays simple.
Part of our high-risk pregnancy care cluster: thyroid is one of the pre-existing conditions we screen for and manage closely before, during, and after pregnancy.

“A thyroid problem rarely arrives with a single dramatic symptom. It usually shows up as a slow drift, less energy, weight that will not move, periods that stopped behaving, hair that has gone thin. When women describe these changes to me, the first thing I do is rule the thyroid in or out. It takes one blood test, and it changes how we plan everything else.”
- Dr. Pallavi Kulkarni
What Is the Thyroid Gland and Why Does It Matter?
The thyroid is a small, butterfly-shaped gland that sits at the front of your neck, just below the Adam’s apple. It produces two hormones, called T3 and T4, that travel in your blood and act on almost every cell in your body. The NHS overview of thyroid disease is a useful plain-English starting point if you want background reading alongside this page.
You can think of these hormones as the body’s pace-setter. They decide how fast your heart beats, how quickly you burn energy, how warm or cold you feel, how regular your periods are, and even how clearly you think. When the thyroid produces the right amount, you barely notice it. When it produces too little or too much, the whole system feels off.
Women are five to eight times more likely than men to develop a thyroid problem, and the risk goes up further during the reproductive years, in pregnancy, and around menopause. That is why every gynaecologist pays close attention to thyroid status.
How Common Are Thyroid Disorders in Indian Women?
The Indian numbers are striking. A large eight-city epidemiological study (which included Mumbai) found that roughly one in ten adults had hypothyroidism, and that nearly a third of those affected had no idea they had the condition. Among women, the rate is consistently higher than men.
Several reasons sit behind these numbers, including iodine intake patterns, genetics, autoimmunity, and how few women get screened until something goes wrong. The practical takeaway is simple: a thyroid test should not feel like a special investigation. It should be a routine part of evaluating fatigue, weight changes, irregular periods, fertility issues, or pregnancy planning.
Sources: Unnikrishnan AG et al., 8-city Indian epidemiological study, Indian J Endocrinol Metab; Yadav V et al., meta-analysis, J Thyroid Research, 2021.
Types of Thyroid Disorders Women Should Know About
Not all thyroid problems are the same. Knowing which one you have changes the treatment plan.
Hypothyroidism (underactive thyroid)
The gland is producing too little hormone. The body slows down. Hashimoto’s thyroiditis, an autoimmune condition where the body’s own immune system gradually damages the thyroid, is the most common cause in Indian women.
Subclinical hypothyroidism
A milder version, where the TSH level is slightly raised but T4 is still in the normal range. Many women have no obvious symptoms at this stage, which is why it gets missed. It often shows up first during a fertility workup or an antenatal blood test.
Hyperthyroidism (overactive thyroid)
The gland is producing too much hormone. The body speeds up. The most common cause is Graves’ disease, also autoimmune in nature.
Postpartum thyroiditis
A temporary inflammation of the thyroid that can occur in the first year after childbirth. It often presents first as hyperthyroidism, then swings into hypothyroidism. Around 5 to 10 percent of women experience some form of it after delivery, and many cases are misread as ordinary postpartum fatigue.
Thyroid nodules
Small lumps inside the gland. The vast majority are non-cancerous, but they should be evaluated with an ultrasound and, in some cases, a fine-needle test.
What Are the Symptoms of a Thyroid Disorder?
Symptoms vary depending on whether the thyroid is underactive or overactive. The list below is not a checklist for self-diagnosis, but if several of these feel familiar, a thyroid test is a sensible next step.
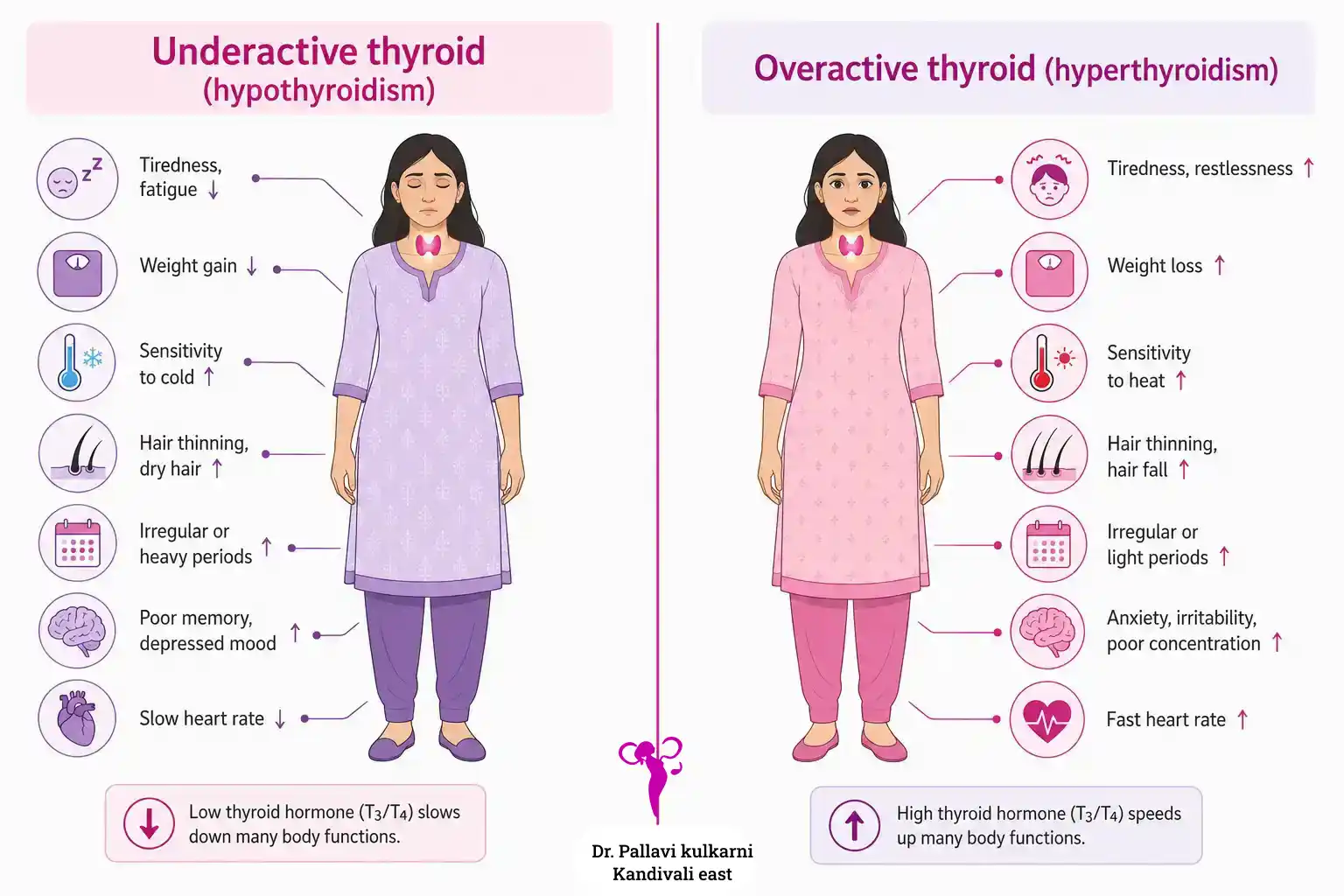
| Underactive thyroid (hypothyroidism) | Overactive thyroid (hyperthyroidism) |
|---|---|
| Constant tiredness, even after a full night’s sleep | Feeling restless, anxious, or on edge |
| Unexplained weight gain or trouble losing weight | Unintended weight loss despite normal eating |
| Feeling cold when others are comfortable | Feeling hot, sweating more than usual |
| Dry skin, brittle nails, hair fall | Hair thinning |
| Heavy or irregular periods | Lighter, irregular, or skipped periods |
| Constipation | Loose stools or frequent bowel movements |
| Low mood, brain fog, poor concentration | Trembling hands, racing heart |
| Puffy face, swelling around the eyes | Bulging eyes, gritty or watery eyes (in Graves’) |
| Slow heart rate | Difficulty sleeping |
Two important caveats. First, all of these symptoms can have other causes - anaemia, vitamin D deficiency, PCOS, depression, or simply being overworked. Second, in subclinical hypothyroidism there may be no symptoms at all. That is why the blood test matters more than the symptom checklist.
“Many of my patients tell me they spent two or three years feeling ‘just a bit off’ before getting tested. The thyroid is one of the easiest things to check and one of the easiest to treat. There is no good reason to live with vague tiredness for years when a single blood test can give you an answer.”
- Dr. Pallavi Kulkarni
Worried about persistent tiredness, weight changes, or irregular periods? A thyroid panel takes one blood draw and can give you clarity within a day.
Thyroid and Fertility: The Hidden Connection
If you are trying to conceive and the months are slipping by, your thyroid is one of the first things worth checking. The link between the thyroid and fertility runs through several different pathways.
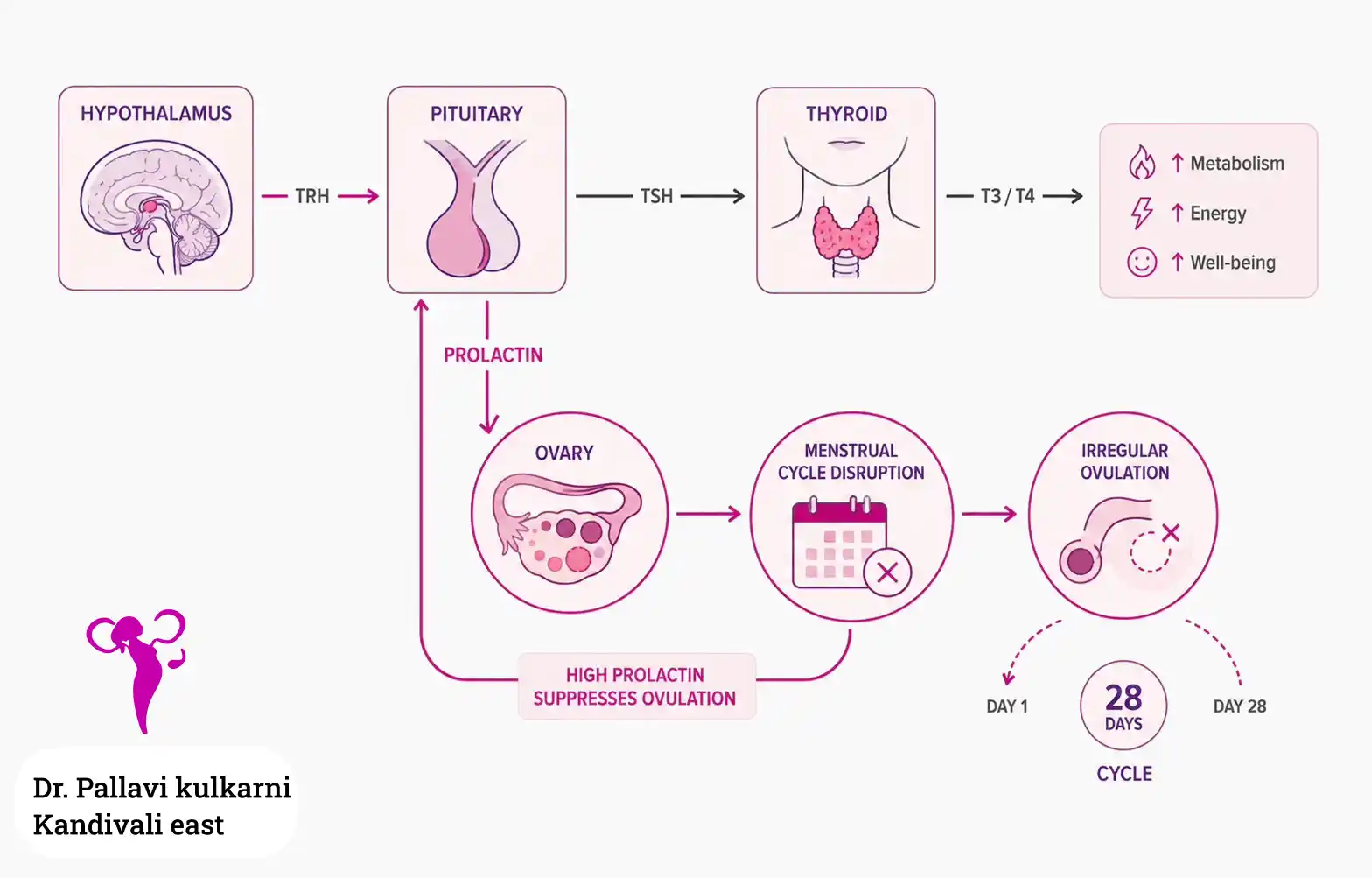
How an underactive thyroid affects ovulation and the menstrual cycle
When thyroid hormone levels drop, the brain compensates by producing more of a signalling hormone called TRH. TRH does its job of asking the thyroid to work harder, but it also nudges the pituitary gland to release more prolactin - the hormone normally associated with breastfeeding. Higher prolactin levels can suppress ovulation, shorten the luteal phase of your menstrual cycle, or stop periods altogether.
This is why women with untreated hypothyroidism often have:
- Irregular periods, frequently heavy or absent
- Anovulatory menstrual cycles - cycles where no egg is released
- A shortened luteal phase, which makes implantation harder
- Higher rates of early miscarriage
How an overactive thyroid affects fertility
Hyperthyroidism is less common but equally disruptive. It can cause lighter or skipped periods and reduce the chances of conception. In pregnancy it carries its own risks, which is why it must be controlled before trying to conceive.
Thyroid antibodies and miscarriage
Some women have normal thyroid hormone levels but test positive for thyroid antibodies (TPO antibodies). This pattern, called thyroid autoimmunity, is associated with a higher risk of recurrent miscarriage and infertility, even when TSH itself looks fine. It is something we evaluate carefully in women with unexplained pregnancy loss, in line with the ASRM 2024 Practice Guideline.
In clinic, a common pattern is that a woman comes in after several months of trying to conceive, with mostly regular periods or subtle menstrual changes. Many patients with thyroid disorders also present with menstrual irregularities, which may range from lighter menstrual flow to heavier bleeding, depending on the thyroid levels and whether the thyroid is underactive or overactive.
Basic fertility tests may look reassuring, but a thyroid panel sometimes shows raised TSH or positive thyroid antibodies, suggesting that the thyroid may be quietly affecting ovulation, cycle quality, or early pregnancy planning. In such cases, the next step is usually not panic, but careful interpretation of TSH, free T4, thyroid antibodies, menstrual pattern, and pregnancy plans, followed by treatment or monitoring where appropriate. Alongside the clinical picture, our Ovulation and Fertile Window Calculator can give a rough estimate of the fertile window in cycles that are still reasonably regular - useful only as a starting point alongside thyroid correction.
The important point is that thyroid testing is a small blood test, but in selected fertility cases it can change the clinical direction meaningfully.
- Dr. Pallavi Kulkarni, on patterns frequently seen in fertility consultations
If you have been trying to conceive for six months or longer without success, or you have had two or more miscarriages, a thyroid panel including TPO antibodies is part of a sensible fertility evaluation.
Thyroid and Pregnancy: What You Need to Know
Pregnancy puts an extra demand on the thyroid. The body needs more thyroid hormone from very early in the first trimester, partly to support the baby’s developing brain. A baby’s own thyroid does not start working properly until around 18 to 20 weeks, so until then, the baby is entirely dependent on yours.
Why thyroid status matters in pregnancy
Untreated or under-treated hypothyroidism in pregnancy is associated with:
- Miscarriage, particularly in the first trimester
- Pre-eclampsia and high blood pressure
- Preterm birth
- Low birth weight
- Reduced cognitive development in the child, especially when hypothyroidism is severe and untreated
The good news is that all of these risks are largely preventable when the thyroid is treated properly during pregnancy. This is why thyroid testing is part of routine antenatal care in our high-risk pregnancy protocol.
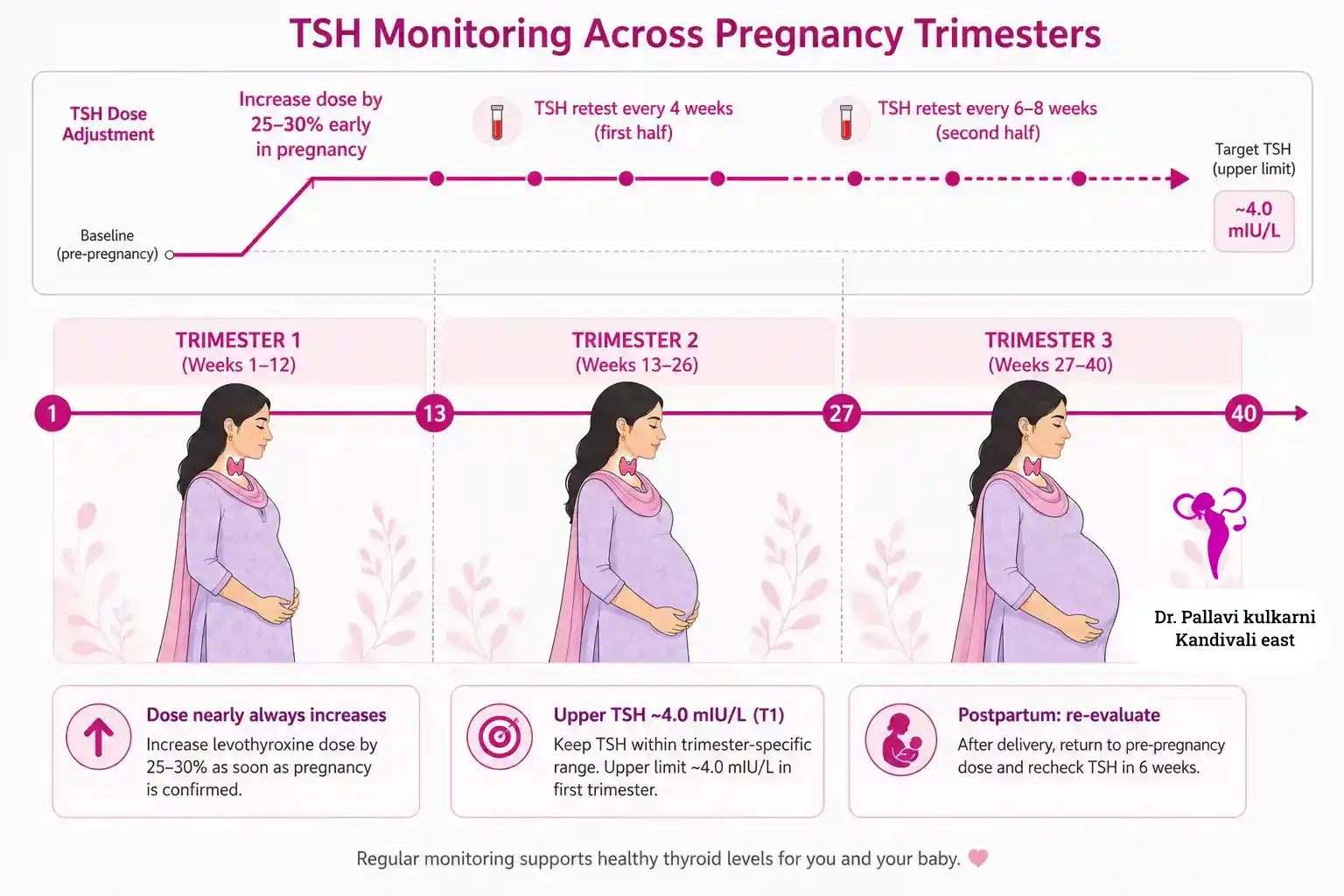
Pregnancy-specific TSH ranges
The reference range for TSH shifts in pregnancy because of changes in the hormone hCG. The 2017 American Thyroid Association guidelines suggest using local trimester-specific ranges where available. Where a local range is not established, the targets below are commonly used.
| Stage | TSH target (per ATA 2017) |
|---|---|
| Pre-conception (trying to conceive) | Below 2.5 mIU/L recommended |
| First trimester | 0.1 - 2.5 mIU/L (upper limit ~4.0 mIU/L acceptable in healthy women) |
| Second trimester | 0.2 - 3.0 mIU/L |
| Third trimester | 0.3 - 3.0 mIU/L |
| Non-pregnant adult women | 0.4 - 4.0 mIU/L (lab-dependent) |
Source: American Thyroid Association 2017 Management Guidelines for Thyroid Disease in Pregnancy and the Postpartum (reaffirmed in subsequent ATA guidance).
Women already on thyroid medication usually need a dose increase early in pregnancy, sometimes by 25 to 30 percent (per ATA 2017, reaffirmed in subsequent ATA guidance), which is why testing in the first few weeks is so important. If you are already on levothyroxine and planning a pregnancy, a pre-conception TSH check is the single most important first step.
Already on thyroid medication and planning a pregnancy?
A pre-conception consultation lets us optimise your TSH before you conceive, review your medication dose, check antibody status, and plan how often to retest once you are pregnant. This is far easier than catching up later. If you are also over 35 and planning a pregnancy, thyroid screening is one of the first things we’ll bring forward.
Postpartum thyroiditis
If you feel unusually anxious, hot, or shaky in the first three to six months after delivery, or unusually tired, low, and cold beyond that, please mention it. These symptoms are commonly assumed to be “normal new-mum exhaustion” and they often are. But sometimes they signal postpartum thyroiditis, which is straightforward to identify and manage.
Planning a pregnancy and unsure whether your thyroid needs checking first? A pre-conception consultation can answer that in a single visit.
How Are Thyroid Disorders Diagnosed?
Diagnosis is mostly a blood test. The tests your doctor may order depend on your symptoms and history.
| Test | What it tells us |
|---|---|
| TSH (Thyroid Stimulating Hormone) | The single most useful test. A high TSH suggests an underactive thyroid; a low TSH suggests overactive. |
| Free T4 (FT4) | Measures the active circulating hormone. Used together with TSH to confirm the diagnosis and tell overt from subclinical disease. |
| Free T3 (FT3) | Sometimes added in suspected hyperthyroidism. |
| TPO antibodies (Anti-TPO) | Detects autoimmune thyroid disease, including Hashimoto’s and Graves’. Especially relevant in fertility and recurrent miscarriage workups. |
| Thyroglobulin antibodies | Sometimes added when autoimmunity is suspected but TPO is negative. |
| Thyroid ultrasound | If a lump or nodule is felt, or if the gland looks enlarged. |
| Fine-needle aspiration | Only for nodules that need further evaluation. |
Most women only need a TSH and Free T4 to begin with. The other tests are added based on what the first results show. Fasting is not required for thyroid tests, and the morning is generally the best time to draw blood.
How Are Thyroid Disorders Treated?
Treatment for hypothyroidism
The standard treatment is a daily tablet of levothyroxine, which is a synthetic version of the T4 hormone your body makes naturally. It is taken on an empty stomach in the morning, ideally 30 to 60 minutes before food, tea, coffee, or any other medication.
A few things to know about levothyroxine:
- It is not a steroid and it is not addictive.
- Most women take it for life, because the underlying cause (often Hashimoto’s) does not reverse on its own. That is normal and safe.
- The dose is small and adjusted based on TSH retesting, usually six to eight weeks after starting or after any dose change.
- Calcium tablets, iron tablets, antacids, and high-soy meals can interfere with absorption. Keep at least a four-hour gap.
- In pregnancy, the dose nearly always needs to go up. Do not adjust it yourself. We retest TSH every four weeks in the first half of pregnancy.
Treatment for subclinical hypothyroidism
This is more nuanced. Treatment is generally recommended when TSH is significantly raised, when TPO antibodies are positive, when a woman is trying to conceive, or in early pregnancy. For mildly raised TSH in women who are otherwise well and not planning a pregnancy, watching and re-testing is sometimes the right call. The decision is individualised.
Treatment for hyperthyroidism
Three main options are used, often in combination:
- Anti-thyroid medication, usually carbimazole or methimazole, to reduce hormone production.
- Radioactive iodine therapy, which reduces the gland’s activity over weeks to months. Not used in pregnancy or breastfeeding.
- Surgery, in selected cases such as very large goitres or suspected cancer.
The treatment plan changes if you are pregnant or planning a pregnancy, since some medications are preferred in different trimesters. This is one of the conversations to have before, not after, conceiving.
How long until I feel better?
Most women on levothyroxine begin to notice improvements in energy, mood, and sleep within four to six weeks of being on the right dose. Hair regrowth, weight, and period regularity often take longer, sometimes three to six months. Patience helps.
What Should I Eat - And Avoid - With a Thyroid Disorder?
There is no diet that cures a thyroid problem. What you eat can either support or interfere with your treatment, but it does not replace medication. The advice below is practical and adapted for an Indian kitchen.
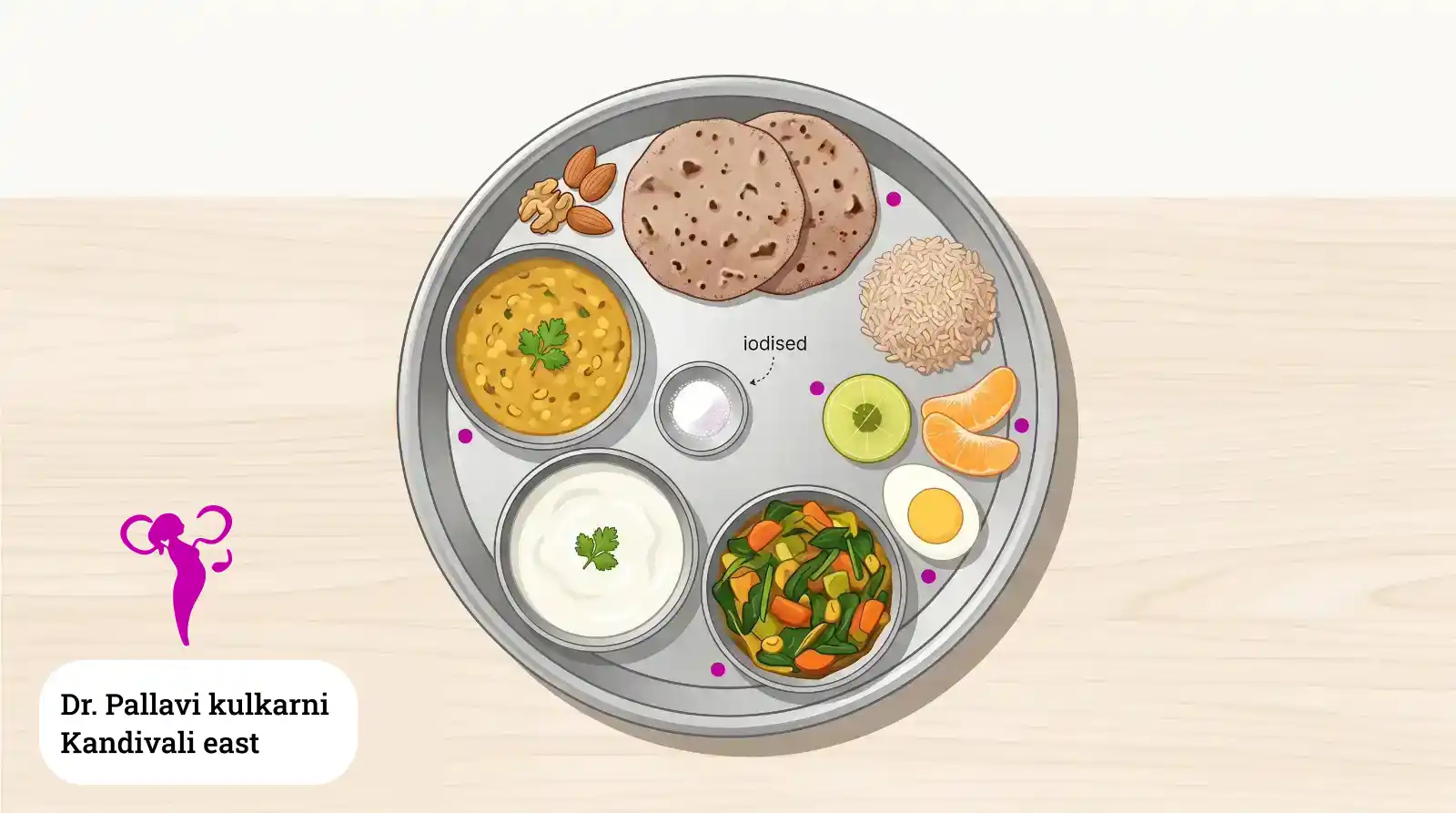
Foods that support a healthy thyroid
- Iodised salt for everyday cooking. The iodine in fortified salt is one of the simplest ways to keep thyroid hormone production steady.
- Curd (dahi) and milk, which provide iodine, calcium, and protein.
- Eggs, fish (when included), and lean meat for selenium and zinc, both of which help the thyroid work efficiently.
- Dals and pulses for plant protein.
- Nuts, particularly two to three Brazil nuts a week if you can find them, for selenium. Otherwise, almonds and walnuts are fine.
- Fruits and vegetables in variety, including amla, which is high in vitamin C.
- Whole grains and millets such as ragi, jowar, and bajra, which have replaced refined grains in many Indian households for good reason.
Foods to time around your medication, not avoid
Some foods do not harm the thyroid itself, but they reduce how well your levothyroxine is absorbed. The fix is timing, not elimination.
- Soy products (soy milk, tofu, soy chunks): keep at least four hours between soy and your morning tablet.
- High-calcium meals or calcium supplements: same four-hour rule.
- Iron supplements and antacids: same.
- Coffee, including filter coffee: wait at least 30 to 60 minutes after taking the tablet.
Foods to be sensible about
- Raw cruciferous vegetables in very large quantities (cabbage, cauliflower, broccoli, kale, radish): these contain compounds that can interfere with iodine use when eaten raw and in excess. Cooking them, even lightly steaming or sautéing, deactivates most of these compounds. A regular helping of sabzi is fine.
- Cassava (tapioca, sabudana flour from cassava): can release thyroid-slowing compounds when undercooked. Stick to well-cooked preparations.
- High-dose iodine or kelp supplements: the American Thyroid Association notes that the recommended daily intake of iodine for adult women is 150 micrograms, rising to 220 to 250 micrograms in pregnancy. Many over-the-counter kelp supplements deliver several times this amount in a single capsule, which can actually destabilise thyroid function. Iodised salt is enough for most women. Iodine supplements should only be taken on medical advice.
A note on rock salt (sendha namak) and pink Himalayan salt
Both are popular, but neither is naturally iodised in the way standard cooking salt is. If you exclusively use rock or pink salt, you may not be getting the iodine your body needs. The simplest fix is to use iodised salt for routine cooking and reserve other salts for fasting days or finishing dishes.
“Patients often ask me whether they should give up wheat, soy, or dairy because of something they read. My answer is usually no, but we do need to think about timing. Take your tablet first thing in the morning with water, wait 30 to 60 minutes, then have whatever you normally eat. That single habit fixes most of the absorption problems people worry about.”
- Dr. Pallavi Kulkarni
When to See a Specialist
Consider booking an appointment if any of the following apply:
- You have noticed several of the symptoms listed earlier and they have lasted more than a few weeks.
- You are trying to conceive, or you have been trying for six months or more without success.
- You have had a miscarriage, particularly more than one.
- You are already on thyroid medication and your dose has not been reviewed in over a year.
- You are planning a pregnancy and you have a family history of thyroid problems, autoimmune disease, or diabetes.
- You are postpartum and feeling unusually unwell beyond the typical fourth-trimester adjustment.
- You have noticed a swelling or lump in the front of your neck.
- You have PCOS, irregular periods, or unexplained hormonal symptoms - thyroid testing should be part of the workup.
Dr. Pallavi Kulkarni evaluates and treats thyroid problems alongside her general gynaecology and obstetric practice at Aarogya Women’s Clinic. Where additional input is needed, she co-manages cases with trusted endocrinologists in the Kandivali and Borivali area.
Clinic hours: Monday to Saturday, 10:00 AM to 9:00 PM · Closed Sundays · Languages: English, Hindi, Marathi
Women from Kandivali East including Thakur Village, Kandivali West, Malad East, Malad West, Borivali East, Borivali West, Goregaon East, and Goregaon West consult Dr. Pallavi Kulkarni for evaluation and management of thyroid disorders in women, with care tailored to fertility plans, pregnancy stage, and the menstrual-cycle changes that often bring patients in.
Dr. Pallavi Kulkarni is registered with the Maharashtra Medical Council, MMC reg. no. 2005/06/2917. She holds an MBBS (KIMS Karad, MUHS), DNB (OB/GYN) (Central Railway Hospital Byculla, Natboard), Fellowship in IVF (AMOGS-MCOG), DGO (CPS Mumbai), DFP (FOGSI), and MRCOG from the Royal College of Obstetricians and Gynaecologists, UK.
Ready to take the next step? Call +91 91366 33062 or message us on WhatsApp to book a thyroid consultation with Dr. Pallavi Kulkarni.
References
- Unnikrishnan AG, Kalra S, Sahay RK, et al. Prevalence of hypothyroidism in adults: An epidemiological study in eight cities of India. Indian J Endocrinol Metab. 2013. PMC3743364.
- American Thyroid Association. 2017 Guidelines of the American Thyroid Association for the Diagnosis and Management of Thyroid Disease During Pregnancy and the Postpartum (reaffirmed in subsequent ATA guidance). thyroid.org.
- American Society for Reproductive Medicine. Practice Committee Documents (2024). asrm.org.
- NHS. Thyroid disease - overview. nhs.uk.
- Mayo Clinic. Hashimoto’s disease - symptoms and causes. mayoclinic.org.
- Cleveland Clinic. Graves’ disease - causes, symptoms and treatment. my.clevelandclinic.org.
- Endocrine Society. Iodine and the Thyroid Gland - patient resources. thyroid.org.
- Royal College of Obstetricians and Gynaecologists (RCOG, UK). rcog.org.uk.
- Federation of Obstetric and Gynaecological Societies of India (FOGSI). fogsi.org.
This page is reviewed periodically by Dr. Pallavi Kulkarni. Last reviewed . Information provided is for educational purposes and not a substitute for professional medical advice.
Do you have any questions?
Request An AppointmentFAQ
Can a thyroid problem be cured?
Most thyroid disorders can be controlled very well with daily medication, but the underlying cause (often autoimmune) does not usually reverse. Many women take levothyroxine for life, in the same way someone with high blood pressure stays on a daily tablet. It is safe, inexpensive, and effective.
Will I need thyroid medication forever?
Often yes, particularly if you have Hashimoto’s or have had thyroid surgery. Postpartum thyroiditis, however, sometimes resolves on its own within 12 to 18 months. The decision to continue, taper, or stop medication is based on repeated TSH testing, not on how you feel.
Can I get pregnant if I have hypothyroidism?
Yes. Hypothyroidism that is properly treated does not stand in the way of pregnancy. The key is getting your TSH into the optimal range before conceiving and keeping it there throughout pregnancy with regular testing.
Is it safe to take thyroid medication during pregnancy?
Yes. Levothyroxine is one of the safest medications used in pregnancy. In fact, stopping it can be harmful for both you and the baby. Your dose will likely need to be increased once you conceive.
Does thyroid cause weight gain?
An underactive thyroid can cause some weight gain, often from a mix of slowed metabolism and water retention. The amount is usually modest, in the range of 2 to 5 kilograms. If you have gained significantly more, other factors are usually also at play, and treating the thyroid alone may not bring all of it back down.
Should I get my thyroid tested if I have PCOS?
Yes. Thyroid disorders and PCOS often coexist, and the symptoms overlap significantly. A TSH test is part of any sensible PCOS workup.
What is the best time to take thyroid medication?
First thing in the morning, with water, on an empty stomach. Wait 30 to 60 minutes before having tea, coffee, or breakfast. Avoid taking it with calcium or iron tablets.
Are home remedies or ayurvedic medicines safe for thyroid?
Some general lifestyle measures - balanced diet, exercise, sleep, stress management - support thyroid health and are always welcome. Specific herbal supplements claiming to cure thyroid problems should be discussed with your doctor first, because some interact with thyroid medication or contain undisclosed iodine doses.
I am vegetarian and avoid dairy. Will I get enough iodine?
It is harder, but possible. Iodised salt remains your main source. Strict vegan diets may benefit from a measured iodine supplement, but only after speaking to your doctor. Avoid high-dose kelp or seaweed supplements bought online.
Does the thyroid affect periods?
Yes. Both an underactive and an overactive thyroid can change cycle length, flow, and regularity. Heavy or absent periods that started or worsened recently are a reason to check your thyroid.
What Our Patients Say
Experienced Gynecologist in Kandivali East with a Patient-Centered Approach
Dr. Pallavi Kulkarni is a highly regarded Gynecologist in Kandivali East, praised for her calm, compassionate, and patient-centered care. Her supportive approach helps women feel heard, respected, and confident about their treatment decisions.